
 فارسی
فارسی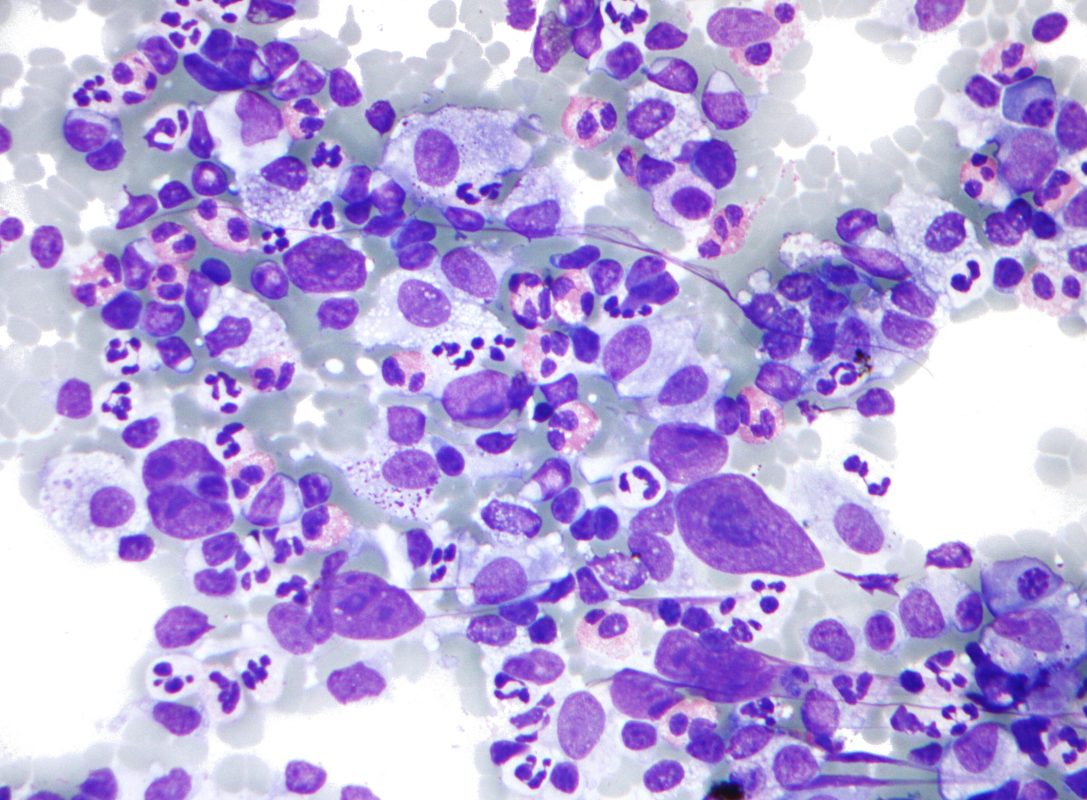
Hodgkin’s lymphoma
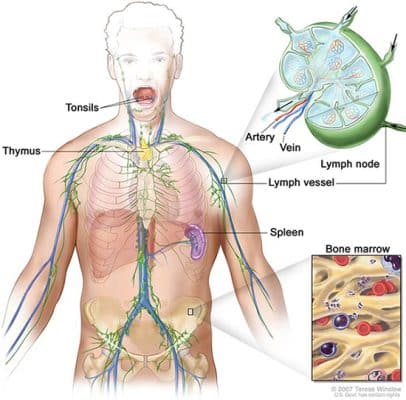
Hodgkin’s lymphoma is a type of cancer of the blood and immune system known as lymphoma, which may affect any part of the body’s lymphatic system, including the lymph nodes, bone marrow, or spleen.
The most common age of its prevalence is in the third decade of life (20-24 years old) and after 55 years old (84-80 years old). This disease is more common in men than women. According to the US National Cancer Institute, it is estimated that in 2023, 80,830 Hodgkin’s lymphoma new cases will be diagnosed. Fortunately, this disease has a favorable prognosis, so that its 5-year survival rate is reported to be 89%.
Classic Hodgkin’s lymphoma accounts for almost 95% of all Hodgkin’s lymphomas. Classic Hodgkin’s lymphoma usually occurs in the lymph nodes of the neck. This lymphoma has an excellent overall prognosis with an almost 80% cure rate. Classic Hodgkin lymphoma has 4 types.
Type 1: Lymphocyte-rich Classic Hodgkin Lymphoma, which has the best prognosis.
Type 2: Nodular Sclerosing Hodgkin Lymphoma: the most common Hodgkin Lymphoma
Type 3: Mixed Cellularity Hodgkin Lymphoma, The subtype most associated with EBV.
Type 4: Lymphocyte Depleted Hodgkin Lymphoma
Many studies have been conducted on the etiology of Hodgkin’s lymphoma, and one of the causes of this disease is infection with the Epstein-Barr virus. Some patients have systemic symptoms. These symptoms include unexplained fever above 38 degrees, weight loss of more than ten percent over the past six months, and night sweats. The stages of the disease are classified into four categories.
Stage 1: Disease is limited to lymph nodes in one anatomical region or two adjacent regions on one side of the diaphragm.
Stage 2: It involves more than two adjacent areas or two non-adjacent areas on one side of the diaphragm.
Stage 3: the involvement is on both sides of the diaphragm, but it is limited to the lymphatic tissue.
Stage 4: it involves the bone marrow or other organs in addition to the lymphoid tissue.
The disease is diagnosed first by clinical examination and then by imaging investigations. If the patient’s CT scan results are suspicious, a sample is taken from the site to be evaluated histologically and to determine the subtype of the disease and its prognosis.
Staging evaluations for a patient with Hodgkin’s lymphoma typically include a detailed history and complete physical examination, CBC test, ESR test, LDH measurement, chest X-ray, CT scan of the chest, abdomen, and pelvis. and bone marrow biopsy. LDH increases in 30-40% of patients in the initial cases of the disease.
After the definitive diagnosis of the disease, the treatment begins. The patient is monitored after each course to evaluate the response to the treatment.
One of treatment option for these patients is autologous stem cell transplantation. However, some people whose disease relapsed and refractory, are candidates for allogeneic stem cell transplantation. It is recommended to start searching for a suitable stem cell donor if the primary evaluation indicate a poor prognosis, from the diagnosis.
Non-Hodgkin’s lymphoma:
This group of lymphomas includes many different subtypes. Some of them involve B cells and some involve T cells. However, most non-Hodgkin’s lymphomas involve B cells. In general, non-Hodgkin’s lymphoma is the eighth most common malignancy in the world, and its prevalence is higher in men than in women.
These lymphomas can be indolent or aggressive. Different subtypes can be distinguished based on immunophenotyping. In addition, some genetic alternation in molecular studies help to differentiate and identify them. Below we explain some of them that have a higher prevalence.
Chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL):
Chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) are characterized by a progressive accumulation of leukemic cells in the peripheral blood, bone marrow, and lymphoid tissues. CLL clinical course is very heterogeneous: the majority of patients follow an indolent clinical course with no or delayed treatment need, and if certain criteria are positive, treatment is started.
Diffuse large B cell Lymphoma (DLBCL):
DLBCL is one of the most common lymphomas and accounts for 35% of lymph node cancers. This disease is very heterogeneous clinically and molecularly. Rituximab is the backbone for the treatment of these patients.
Following chemotherapy, autologous stem cell transplantation can improve the outcome many patients. According to the statistics of the National Cancer Institute, the 5-year survival rate of this disease is about 65%.
Follicular lymphoma
Follicular lymphoma is characterized by diffuse lymphadenopathy, bone marrow involvement, and splenomegaly. This lymphoma is often indolent (slow-growing.) The prevalence of this lymphoma is approximately equal between men and women.
The average age of patients at the time of diagnosis is 64 years. According to the National Cancer Institute, the 5-year survival rate of this disease is about 91%.
Burkitt’s lymphoma
It is closely related to L3 acute lymphoblastic leukemia (FAB classification) and is seen endemically or sporadically. Endemic Burkitt’s lymphoma is usually seen in areas where there is chronic contact with the malaria parasite.
This disease is also related to the EBV virus. In almost all cases, we see the manifestation and overexpression of the C-MYC oncogene, which is due to the placement of this oncogene in the immunoglobulin gene kinase as a result of the translocation of chromosomes eight and fourteen ( t(8:14) ). Patients are usually children who have prominent lymphadenopathy in jaws, abdomen, neck, or head.
Mantle cell lymphoma:
It is a rare subtype of non-Hodgkin’s lymphoma. t(11:14) is one of the hallmark of this lymphoma. The clinical course of mantle cell lymphoma is aggressive.
MALT Lymphoma:
Clinical trials revealed the important role of Helicobacter pylori (H. pylori) in the pathogenesis of gastric MALT lymphoma. In the early stages, treatment with antibiotics to eliminate Helicobacter pylori can be effective in treating this disease. it can be easily misdiagnosed because of unspecific symptoms of the digestive tract.
Author and translator: Dr. Farzaneh Tavakoli
Read more:
Selection of sources: