
 فارسی
فارسی
Allogeneic hematopoietic cell transplantation (allo-HCT) is a curative therapy for hematologic disorders, but its success is complicated by graft-versus-host disease (GvHD). Since allo-HSCT requires conditioning, tissue damaging events will occur in all patients undergoing this procedure.
Chemotherapy and radiotherapy used during the conditioning regimens induce tissue damage and consequently release exogenous and endogenous molecules that activate the innate immune response.
The ultimate results of these events are GvHD. GvHD is an adverse immunologic phenomenon following allogenic hematopoietic stem cell transplant. There are two main types of GvHD- acute (aGvHD) and chronic (cGvHD)-differing in the pathogenesis, time of onset, and clinical presentation.
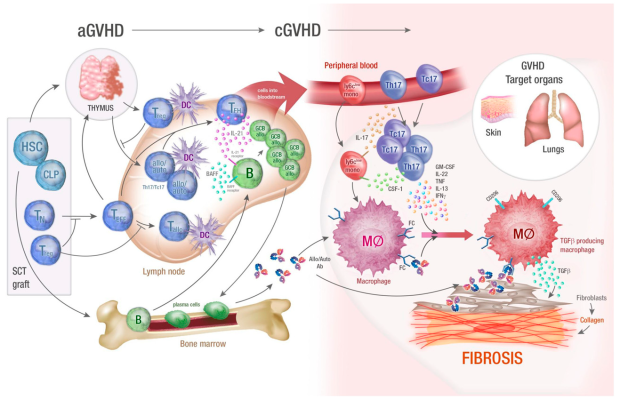
the incidence of aGvHD is approximately 30%-50%. This condition usually occurs within the first 3 months after alloHCT, but later onset is possible. In phase 1, conditioning chemoradiotherapy induces tissue damage and the release of inflammatory cytokines.
In phase 2, activation of donor T cells leading to their clonal expansion and differentiation. In phase 3, Such activation leads to the release of inflammatory cytokines, with subsequent proliferation of alloreactive T cells, resulting in host damage and inflammation.
Acute graft-versus-host disease (a-GVHD)
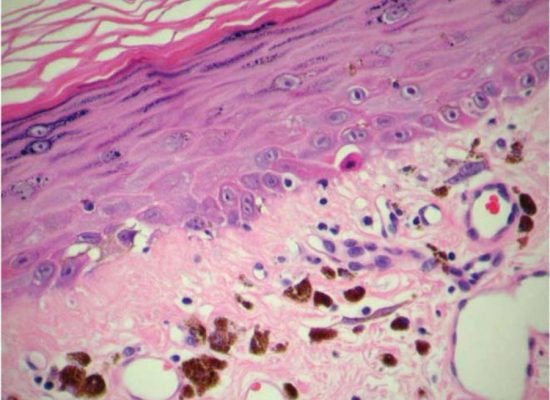
aGvHD usually presents with either maculopapular erythematous skin rash, gastrointestinal (GI) toxicity (nausea, vomiting, diarrhea, GI bleed, ileus, weight loss, abdominal pain), hyperbilirubinemia or a combination thereof. Imbalances in the gut microbiota are also likely to have a significant role in the development of aGvHD of the gastrointestinal tract.
Only half of patients with aGvHD respond to first-line treatment with corticosteroids. Ruxolitinib, an oral selective JAK1/2 inhibitor, received Food and Drug Administration (FDA) approval for the treatment of steroid-refractory aGvHD in 2019 and remains the only agent approved for aGvHD.
Chronic graft-versus-host disease (GVHD)
cGvHD is the leading cause of late morbidity and mortality after allo-HCT. Occurring a minimum of 100 days following stem cell transplantation, around 50% of patients will experience some degree of cGvHD.
Historically, alloreactive donor T cells have been the primary factor implicated in the pathophysiology of cGvHD. Risk factors for cGvHD development include recipient age, prior aGvHD, donor peripheral blood stem-cell grafts, HLA disparity and female donors for male recipients. Every phase of cGvHD involves a diverse set of immune cells, which exert several disease-promoting pathomechanisms.
Its diagnosis is complicated. While cGvHD has been previously defined by its time of onset (more than 100 days after BMT), it is now classified on the basis of clinical diagnostic features. Commonly targeted organs are skin, eyes, mouth, gastrointestinal tract, and liver. Global severity scoring is divided into mild, moderate, or severe based on the number and severity of involved organs.
Mild forms of chronic GvHD are often manageable with local or low-dose systemic immunosuppression and do not affect long-term survival. Moderate-to-severe cGvHD is associated with poor health-related quality of life and crucial disease burden. Severe cGvHD is the cornerstone reason for morbidity and mortality in long-term survivors of alloHSCT. The current standard first-line cGvHD therapy is glucocorticoids. There are currently 3 FDA approvals for cGvHD management: (1) ibrutinib, (2) belumosudil, (3) ruxolitinib.
Compiler and translator: Dr. Farzaneh Tavakoli
Selection of sources:
Link 1
Link 2